Case Study
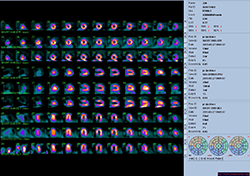
Top row stress supine. Middle row stress prone. Bottom row rest supine. Courtesy of Midwest Heart & Vascular Specialists.
WBR: Xpress3.cardiac rest/stress image
Low-dose isotope imaging study
Rest Dose and scan time: 5.8 mCi Tc-99m sestamibi, scan time 10 minutes.
Stress Dose and scan time: 19.9 mCi Tc-99m sestamibi, scan time 6.5 minutes supine and 4 minutes prone
Type of Stress Test: Treadmill Bruce Protocol for 8 minutes
Achieved 94 % MPHR
Test end due to fatigue
 Patient Data
Patient Data
65-year-old female, 5’5”, 170 lbs. Coronary artery disease (CAD) risk factors: atherosclerosis, hypertension, hyperlipidemia and family history of CAD. Indication for test: syncope.
WBR images acquired with Cardio MD dual-head camera and presented on a Jetstream workstation.
Midwest Heart & Vascular Specialists: Enhancing Image Quality, Patient Care With Xpress.Cardiac
Midwest Heart & Vascular Specialists, Overland Park, Kansas, remains on a mission of providing residents of the Kansas City area with the highest possible caliber of cardiac care and patient experience close to home. Stephen A. Bloom, MD, FACP, FAHA, FACC, FSCCT, FASNC, and his colleagues have long carried out this mission, in part, through quality imaging—which for the practice entails following a protocol that combines prone imaging with supine imaging rather than relying on the latter alone.
“We favor ‘proning’ for the better, easier-to-interpret images it produces,” Bloom said. “We started conducting studies this way before it became a standard practice and have been doing so for more than a decade.”
However, the dual prone-supine protocol initially posed a challenge. Additional time was needed to complete each study, making the procedure less comfortable for patients. Additionally, images captured with patients lying supine were not always reliable from a diagnostic standpoint: When imaging occurs in the supine position, attenuation artifacts—such as those of the breast anteriorly or the diaphragm inferiorly—render it difficult to distinguish between normal and abnormal findings.
Saving Time, Normalizing Images
To address these problems as well as to offer the highest level of patient care, Midwest Heart & Vascular Specialists implemented UltraSPECT’s Xpress.Cardiac solution, which like all UltraSPECT products leverages the company’s patented WBR technology. WBR differs from other SPECT reconstruction technologies in that it does not assume the photon rays identified by the detector crystal to be perpendicular to it. Rather, it uses an intelligent, accurate iterative image reconstruction process that enables simultaneous resolution and contrast recovery, coupled with noise suppression based on an accurate physical modeling of the photon emission and detection. This enables the model to compensate for the “beam spread function” effect of the equipment’s collimator component, and to automatically adjust for distance from the patient. The end-result: a dramatic reduction of image acquisition time.
“With Xpress.Cardiac, we can complete the prone imaging quickly because it extends the entire study by only an extra four minutes (four-minute non-gated process), so it’s easy for patients,” Bloom said. Just as important, in those extra four minutes, technicians can obtain images that are easier to interpret, because prone imaging helps to correct the register if attenuation is present. Normalization is automatic. According to Bloom, it all adds up to enhanced patient care and a better patient experience.
Lower Doses, Enhanced Safety
For Midwest Heart & Vascular Specialists, Xpress.Cardiac also supports high-quality patient care and a positive experience by eliminating the need—in certain cases—to make the trade-off between high image resolution and the image sensitivity that comes with utilizing gamma cameras. The use of a stress-only protocol on patients who have syncope, are at low to intermediate risk of coronary disease, or have had a stent implanted without having suffered a myocardial infarction represents a key example, according to Bloom. In these cases, instead of decreasing image acquisition time, the solution allows patients to undergo the test after having been administered one-quarter to one-half of the traditional radiopharmaceutical dose. The iterative image reconstruction process harnessed by WBR makes the lack of compromise possible.
Conversely, with gamma cameras, the collimator geometry required to produce high-resolution images (namely long-bore, small-hole, and thick-septa collimation) limits the number of photons reaching the detector crystal to those that are nearly perpendicular to it, resulting in lower image sensitivity. The more limiting the collimators, the higher the image resolution—but as resolution improves, sensitivity is compromised and must be compensated for with increased radiopharmaceutical doses and/or longer acquisition intervals.
“Because the solution works the way it does, we can get a supine and prone view on stress tests with a lower radiopharmaceutical dose,” Bloom noted. “The lower dose in nuclear medicine provides for the flexibility and is a safer, more appealing option for patients.”
Xpress.Cardiac is also a highly viable solution for practices and hospitals whose hardware and software capabilities would otherwise compel them to choose between obtaining high-caliber, high-resolution images (and therefore adding imaging time) and conducting imaging studies at lower radiopharmaceutical doses (and grappling with reduced image sensitivity) for cardiac imaging.
“There are more than 3,000 SPECT/CT scanners in the U.S. today, and most of them are at least five years old,” he explained. “A new machine with both capabilities costs $300,000 to $500,000. Most hospitals—and practices like ours—can enhance image quality and/or lower radiopharmaceutical doses with UltraSPECT at a fraction of that price.”