 Patient is at the Heart of Nuclear Medicine Imaging
Patient is at the Heart of Nuclear Medicine Imaging
Strengthening the Low Dose Message in Nuclear Medicine through Patient Education
The Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting, June 6-10, is just around the corner, and I am looking forward to the annual opportunity to meet and greet UltraSPECT’s old friends, as well as make introductions to newcomers in the field and those we have not yet met. As I was taking a look at what is in store for us at the Baltimore Convention Center, I saw that the SNMMI Patient Advocacy Advisory Board will hold its third Annual Patient Education Day on June 7. Topics range from introducing the patient to the field of nuclear medicine to zeroing in on cardiac, thyroid and brain imaging. One of the main topics is, naturally, what the patient has to know about radiation in nuclear procedure.
Attendance has been growing for the SNMMI patient education sessions, and it is clear that the SNMMI, various patient advocacy organizations in the U.S., and nuclear medicine professionals take seriously the need for educating the patient about molecular imaging and its vital diagnostic and therapeutic roles.
But today’s patients also take an active role in their medical education through research, participation in seminars such as SNMMI’s and by questioning medical solutions presented to them. Naturally, as they learn about what nuclear medicine is and how it works, one of the first questions they ask is “how high is my dose?” and “what does that mean for me?” Likewise, the UltraSPECT team has been predicting this development for some time now.
While the nuclear medicine industry is well aware of the high-dose concern and has been taking measures to lower it – both the SNMMI and the American Society of Nuclear Cardiology (ASNC) have clear recommendations for reducing dose at the point of procedure – we do not have a mandatory standard we must follow. Could an informed patient demanding the lowest possible dose help propel us toward a more unified acceptance of this worthy initiative?
Knowledge is power, and so I commend the SNMMI and everyone else in our field who makes patient education part of their mission. Whether we talk about nuclear medicine imaging techniques to diagnose cardiac disease or explain imaging protocols to patients, the question of the dose will always be present. Let us make the best of this opportunity to empower patients to become their own health –and low-dose – advocates.
The truth is lowering the dose does not require too much effort. Let me recommend an excellent article, “The multi-pronged approach to reducing MPI dose”, in Health Imaging magazine. It gives several recommendations on how to reduce dose in myocardial perfusion imaging and suggests that such effort could reduce the risk of downstream cancers. Dose-reduction approaches such prioritizing patient selection and optimizing procedures can be implemented now.
I’d like to add that several approaches can be taken without extra costs typically associated with purchasing new myocardial perfusion SPECT scan equipment. As a low-cost solution, some facilities implement a stress-only imaging protocol. While both the stress and rest parts of the exam are necessary, certain cases allow for stress-only part of the study to deliver necessary information. As a result, radiation dose is cut in about half. However, attenuation correction is necessary for high-quality stress-only imaging and only a few labs have this capability.
The article mentions image-reconstruction techniques to lower the dose, and UltraSPECT is the pioneer in this cost-effective method, with more than 450 units installed in over 300 health systems across the country.
At the UltraSPECT booth at the SNMMI, we will have our Xpress.Cardiac™, Xpress3.Cardiac™ and Xpress/Xact.Bone™ solutions. Whether imaging at half or quarter time or simultaneously at half dose and half time, physicians and technologists will have images as good, if not better, than those provided with traditional SPECT acquisition. Patients will benefit from safer and shorter scans and increased comfort.
I invite all of you to read the Health Imaging article and think about the approach that will allow you to deliver low-dose, high-quality imaging services to your patients. Stop by our booth # 517 if UltraSPECT sounds like a good fit for your needs.
See you in Baltimore!
Get a Move on for a Good Cause! Take Part in the New “Hot Trot 5K” Run/Walk
 If you are attending the Society of Nuclear Medicine & Molecular Imaging (SNMMI) annual meeting this year, make your visit fun and healthy while supporting a great cause: the SNMMI Technologist Quality Initiative! Run, take a walk or just get out in the sunshine in the beautiful inner harbor together with your peers as part of the new “Hot Trot 5K” run/walk organized by the SNMMI. UltraSPECT is a gold sponsor of the event.
If you are attending the Society of Nuclear Medicine & Molecular Imaging (SNMMI) annual meeting this year, make your visit fun and healthy while supporting a great cause: the SNMMI Technologist Quality Initiative! Run, take a walk or just get out in the sunshine in the beautiful inner harbor together with your peers as part of the new “Hot Trot 5K” run/walk organized by the SNMMI. UltraSPECT is a gold sponsor of the event.
The proceeds from the event will go toward the advancement of molecular and nuclear medicine technologists through professional development that promotes clinical excellence and optimal patient outcomes via the SNMMI-TS Professional Development and Education Fund. Additionally, a portion of the registration proceeds will support a local charity, House of Ruth. The event is scheduled for Saturday, June 6, at 7:30 a.m. in Baltimore, Md.
Online registration is open until May 31 or until the race sells out (whichever comes first). After that date, you can register in person on June 5 or June 6. To sign up, go to the registration page or visit the event Facebook page.
UltraSPECT at the SNMMI Annual Meeting
UltraSPECT is looking forward to another great SNMMI show and will present our most cost-effective and vendor-neutral low dose and ultra-low dose nuclear medicine imaging solutions at booth #517.
Please stop by to say hello and to learn more about how Xpress.Cardiac, Xpress3.Cardiac and Xpress/Xact.Bone solutions provide value to physicians, technologists, patients, administrators and radiopharmaceutical suppliers.
Whether imaging at half or quarter time or simultaneously at half dose and half time, physicians will have superior quality images. With low dose imaging, technologists will benefit from safer and shorter scans, increasing patient comfort, and may also be able to increase the patient throughput in a laboratory without changes in the existing workflow.
Five Questions with James Reibsane, CNMT, Director of Diagnostic and Technical Services at Berks Cardiologists, Wyomissing, Penn.

Q: How did you develop your interest in nuclear medicine (NM)?
A: I studied nuclear chemistry at the University of Nebraska Medical Center and also had a job at a small research reactor for a year in 1980. One day they sent me to the Nuclear Medicine department to survey a spill. As I walked by the rectilinear scanner room, I saw the image of a body on the P-Scope and thought that was the spill! The staff there happily spent the next hour showing me around and explained how they purposely injected isotopes into the patient to take images. It was then that I understood the application of nuclear medicine to help people, and the rest is history.
Q: Why is low dose needed in NM?
A: If you develop a good low-dose protocol that fits your lab and stick to it, it benefits everyone. The patients receive a lower dose, spend less time in the lab and have a higher quality study due to less motion since they spend less time on the camera.
The technologists benefit from less exposure. The nuclear pharmacy has more product when the supply is limited. The practice in general benefits because, if needed, it can add more patient slots without having to purchase another camera.
We have been using UltraSPECT Xpress3.Cardiac™ solution since 2013 and maintain a fairly efficient protocol to produce consistent image results. Lower radiation dose has always been our primary concern. Shorter exam times and not having to change protocols was a side benefit of implementing the technology.
Q: How did the acquisition of UltraSPECT impact your patient care?
A: Patients, especially those with difficulty lying for extended periods, definitely appreciate the shorter scan times. We have some patients who work in the nuclear medicine field and are exposed to isotopes. They already know about the dose and are concerned about how the test would impact their overall radiation dose. They are pleased to know the dose is reduced at our facility.
Many patients asked about the dose after reading about medical radiation exposure during imaging in the media and were impressed that we have already implemented reduced-dose equipment.
Overall, our average patient is much more aware of the dose today than in the past. Patients used to accept medical solutions offered to them but now they do research before they even get in the door of an imaging lab. We need to be better prepared to answer their questions in layman terms to help educate them first-hand.
Q: Is there anything that you perceive as a barrier to adoption of low-dose image-reconstruction techniques in the industry?
One barrier I can see is quantifying the return on investment as there is no reimbursement for this technology. It may not be so easy to quantify the return despite the obvious benefits of the reduced dose to the patients and technologists and better quality images. However, I can say that UltraSPECT technology has certainly helped us during shortages when our nuclear pharmacy needed to reduce activity or deliver Tl-201. UltraSPECT's universal camera capability makes it an easy choice as it works with all types of cameras.
Additionally, a busy lab that consistently has a high patient volume and needs to add patient slots can see an immediate and easily quantifiable return as it increases patient throughput due to reduced scan times.
These days, imaging labs often make investments to continue bringing value to the patient and referring physician in the ever-changing environment. Insurance companies often recommend that other modalities be used first to try to get diagnostic information, though it is a nuclear medicine test that will ultimately provide all the necessary data. We try to bring value to the process by using advanced technology and adding modalities that are relevant and enhance patient care, such as UltraSPECT’s low-dose technology, cardiac PET imaging instead of SPECT for heavier patients, and echo and vascular equipment.
Q: Tell us something about you that few reading this would know.
A: It was difficult for me to make a choice about my career. I had two applications in my hand: one for a nuclear medicine school and one for a clown school in Sarasota Florida. I had a moment when I asked myself what my parents would say... nuclear medicine won. I still rode my six-foot unicycle and juggled until a few years ago.
A Case Study: Half-Dose Half-Time Tc-99m Sestamibi Cardiac Study
UltraSPECT WBR: Xpress3.Cardiac.
Patient Data: 63-year-old male, 5'11'', 175 Ibs.
History: Suspected coronary disease.
Patient diagnosis: Uniform myocardial uptake, normal study, EF=58%.
Clinical Protocol: Tc-99m Sestamibi Single-Day Rest/Stress Myocardial Perfusion Study.
Dosage: 6 mCi, Rest; 20 mCi Stress.
Scan times: 8.5 min. (15 sec/frame) Rest, 6 min. (10sec/frame) Stress.
Half-Dose Half-Time WBR study (Xpress3.Cardiac)
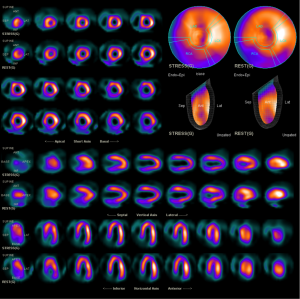
Courtesy of Midwest Cardiologists, Overland Park, KS.
