 Enterprise Imaging, Dose Reduction & A Date with Destiny
Enterprise Imaging, Dose Reduction & A Date with Destiny
Although the chilly winds of Chicago are a significant part of the memory, there were many other notable highlights that came out of the Radiological Society of North America's (RSNA's) 100th Scientific Assembly and Annual Meeting as well. For me, however, two of the popular topics resonated in particular.
The first of the two is enterprise imaging, which was heavily discussed throughout the show. We are experiencing a time where many hospitals are acquiring imaging centers. With each acquisition comes a facility that has its own particular technologies and systems, providing hospitals with a challenge in getting these new additions, along with its existing network, onto the same page in terms of functioning collaboratively. Integration is critical – and PACS systems, viewing stations, CAD systems and support systems must be able to gather information from all modalities of all departments to operate efficiently. A single, completely unified imaging platform enables the archiving, reporting, advanced image processing and integration of all clinical information. Understandably, for high performance results – the imaging workflow must be standardized across the entirety of the hospital’s network.
The second topic is dose reduction – a topic that saw greater awareness than ever before during RSNA. Discussions highlighted the need to lower radiation dose for safer imaging and showcased the ways technology was enabling the reduction of dose by 60 to 80 percent – and even 85 percent in CT systems.
The reason these topics resonated beyond others is simple: they have been the two primary guiding principles for UltraSPECT for nearly a decade. For the nuclear medicine departments with different facilities that they hope they can integrate and bring onto a singular platform with a unified protocol, UltraSPECT was designed to be the answer. Our solution does just that – for all cameras and workstations, regardless of type, age or workflow practice. As far as dose reduction, UltraSPECT’s ability to cost-effectively mitigate radiation risk is unparalleled. There are a few reasons why this matters:
- The Health Physics Society recommends against quantitative estimation of health risks below an individual doses of 50 millisievert (mSv) in one year or a lifetime dose of 100 mSv above that received from natural sources.
- Doses from natural background radiation in the United States average about 3 mSv per year. A dose of 50 mSv will be accumulated in the first 17 years of life.
- Radiogenic health effects (primarily cancer) have been demonstrated in humans through epidemiological studies only at doses exceeding 50–100 mSv delivered at high dose rates. Exposure to relatively low doses delivered over period of time (more than 50 mSv per year) increases the risks of health effects (less than 100 mSv).
- Nuclear Medicine procedures are associated with high levels of radiation (12mSv full R&S MPI), which increases the risk for both caregivers and especially their patients.
Ionizing radiation is used daily in hospitals and clinics to perform diagnostic imaging procedures, of which gamma rays are the most common form. It’s worth acknowledging that the valuable information yielded by such procedures ensures that appropriate care is delivered to patients, while physicians and techs are trained to use the minimum amount of radiation necessary. Still, the below table illustrates a comparison of the dose patients receive when undergoing a procedure with and without UltraSPECT.
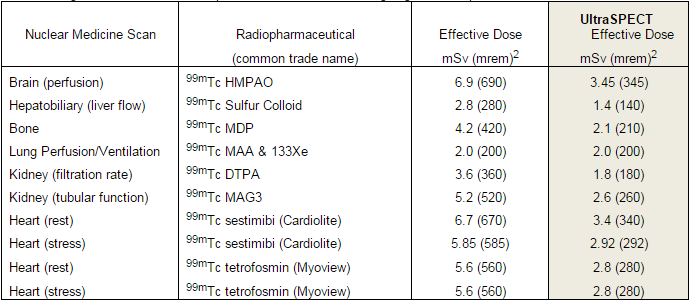
UltraSPECT’s low dose solution can reduce radiation exposure by over 50 percent – something that physicians and technologists can get behind, for both their patients as well as themselves.
Overall, RSNA indicated the medical imaging industry has just now begun to search for what our technology has been providing for years: integration and lower radiation dose. You might say we have a date with destiny – because the time for UltraSPECT is now.
We are excited for the things to come in 2015. Until then, we wish you a wonderful holiday season and a happy new year!
Regards,
Yossi
UltraSPECT in the News
Freedom to Prosper, Through Low Dose, DOTmed Healthcare Business News, November 12, 2014
UltraSPECT Announces Support of HeartLight's HeartSafe Imaging(TM) Initiative, PharmacyChoice, November 25, 2014
UltraSPECT backs HeartSafe Imaging, AuntMinnie, November 27, 2014
Partnership Update

Universal Medical Resources takes great pride in offering new and refurbished nuclear medicine systems, high-quality certified parts, expert repair services, and certified training programs.
Universal has strengthened its support for safer and more thoughtful patient care by forging a partnership agreement with UltraSPECT.
By combining UltraSPECT’s advanced reconstruction solutions with the advanced nuclear imaging cameras, Universal provides nuclear medicine departments with a remarkable package that allows their patients to receive high-quality diagnostic services with significantly reduced dose.
5 Questions with Dan Basso
 Meet one of UltraSPECT’s happy customers, Dan Basso, CNMT, NCT, Director of Cardiovascular Imaging Services, University Health Care System, Augusta, Ga. During a career that has spanned decades, he reflects on how care has advanced significantly.
Meet one of UltraSPECT’s happy customers, Dan Basso, CNMT, NCT, Director of Cardiovascular Imaging Services, University Health Care System, Augusta, Ga. During a career that has spanned decades, he reflects on how care has advanced significantly.
How has the field of nuclear cardiology evolved over the course of your career?
When I helped open Cardiac Imaging Center of Augusta in 1989, we were one of the first nuclear cardiology offices. We saw nuclear cardiology being performed by nuclear medicine physicians or radiologists, then saw cardiologists performing studies, eventually in their own offices. Now we’ve done a 180 and all of those cardiology practices are being brought back into the hospital setting. We’re doing more and more nuclear cardiology as a provider-based rather than practice-based service. That’s really changed the way a lot of nuclear medicine technologists work, which has had a huge impact on the field.
But the most significant shift is the paradigm toward patient-centered care. We’re really improving the care of our patients by doing the right studies on the right patients. We’re able to look at appropriate use criteria, while the software enables delivery of lower dose.
We really shouldn’t have a one-size-fits-all type process for myocardial perfusion imaging. Sometimes, patients would benefit from half dose, while others may need a full dose for half time. Today, we’re able to customize our care and really treat our patients as individuals.
Currently, I’m involved in the development of a new e-book for technologists that will be released by the Society of Nuclear Medicine and Molecular Imaging Technologist Section that will look at quality assurance and methods of lowering dose in myocardial perfusion imaging. The goal of the electronic textbook is to provide an education for technologists in efforts to improve overall patient care in nuclear medicine.
How did you first engage with UltraSPECT technology?
I started to play with it when one of my colleagues asked me to try out the technology. Then, we actually decided to do a study because it was hard to believe that the solution would work – or that half-time imaging was even possible. It goes against the nature of everything we believe. In nuclear medicine, we’re looking at an industry that has been doing what they do the same way for over thirty years – it’s certainly easier to choose to standardize the dose exposure across all patients rather than getting dialed in and providing the most appropriate care to each individual patient.
So, with UltraSPECT, we decided to conduct a study where we would do the full-time imaging first, then repeating the patient again with half-time imaging. We had three nuclear cardiologists read the report, blinded to what was used – and we clearly saw the confidence level and image quality rise with the half-time UltraSPECT imaging.
I did an abstract for the Society of Nuclear Medicine and we actually had the study published in the Journal of Nuclear Medicine Technology (JNMT) in 2009. The paper also went on to also receive 2nd place on the journal’s list of best papers of the year. That was the beginning – it was very exciting and we believed in it. Our physicians also felt like they were seeing more disease than they had previously, and were shocked at the quality of images.
In the several presentations I’ve given over my years in this industry, I’ve discussed ways to lower dose, Image Wisely/Image Gently and more, with the patient always being the primary focus. UltraSPECT can be a powerful tool in patient-centered care delivery – so patients receive the right test, executed in the best way, to deliver the best possible diagnostic benefits while minimizing radiation exposure. Simply put, that is just the direction healthcare is headed.
What technological innovation will most impact nuclear cardiology in the near future?
The biggest thing for nuclear cardiology that’s coming is measuring coronary flow reserve. We can do a pretty good job measuring it with PET right now, and we are moving toward doing that with low energy isotopes as well. This is becoming an important diagnostic tool that will continue to keep nuclear cardiology on the forefront of modern medicine.
What issue has been most challenging for you in practicing or managing medicine?
I’d say health care in general hasn’t really settled out yet. We’ve gone through some huge changes and we’ve had some large swings, and everybody reacts to those swings. Sometimes, we overreact. So hopefully what’s going on in health care will all settle out and we will find the comfortable ground of what medicine is supposed to be. Hopefully, it will improve the care we’re able to provide to our patients.
Taking a step back from work, what’s your favorite family tradition this time of year?
 One of the coolest things that we’ve done with our kids over the years is go camping every Thanksgiving with one main requirement: we cook everything outside over an open fire. So, I make a “trashcan turkey,” Dutch oven style. It’s a lot of fun to challenge the kids, who are now 19 and 15 years old, to get outside and figure out how we were going to cook all of this food. We always have a great Thanksgiving Day dinner – even if we’re in below freezing temperatures or in the midst of a windstorm, we get it done!
One of the coolest things that we’ve done with our kids over the years is go camping every Thanksgiving with one main requirement: we cook everything outside over an open fire. So, I make a “trashcan turkey,” Dutch oven style. It’s a lot of fun to challenge the kids, who are now 19 and 15 years old, to get outside and figure out how we were going to cook all of this food. We always have a great Thanksgiving Day dinner – even if we’re in below freezing temperatures or in the midst of a windstorm, we get it done!
